
More Information
Submitted: February 28, 2025 | Approved: March 24, 2025 | Published: March 26, 2025
How to cite this article: Khanam U, Abid, Kumbar BV. Regional Anesthesia Challenges in a Pregnant Patient with VACTERL Association: A Case Report. Int J Clin Anesth Res. 2025; 9(1): 010-012. Available from:
https://dx.doi.org/10.29328/journal.ijcar.1001027
DOI: 10.29328/journal.ijcar.1001027
Copyright License: © 2025 Khanam U, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: VACTERL; Regional anaesthesia; Pregnancy; High risk

Regional Anesthesia Challenges in a Pregnant Patient with VACTERL Association: A Case Report
Uzma Khanam1*, Abid2 and Bhagyashri V Kumbar2
1Junior Resident, Department of Anaesthesiology, SNMC & HSK Hospital and Research Centre, Bagalkot, India
2Assistant Professor, Department of Anaesthesiology, SNMC & HSK Hospital and Research Centre, Bagalkot, India
*Address for Correspondence: Dr. Uzma Khanam, Junior Resident, Department of Anaesthesiology, SNMC & HSK Hospital and Research Centre, Bagalkot, India, Email: mujeeb_93@yahoo.com
VACTERL (V: Vertebral anomalies, A: Anal malformation, C: Cardiac defect, TE: Tracheoesophageal malformation, R: Renal anomalies, L: Limb anomalies) is a cluster of congenital malformations. It is a rare association with sporadic and non-random occurrence where multiple organs are affected due to developmental defect during blastogenesis (2-4 weeks of gestation), where abnormal structures are derived from the embryonic mesoderm. Multiple environmental and genetic factors have been implicated. We report the successful management of a patient with VACTERL association born to a mother through an emergency cesarean section due to fetal distress.
VACTERL association is a rare and complex congenital disorder characterized by the presence of anomalies in at least three organ systems [1]. The incidence of VACTER association is estimated at 1 in 10,000 to 1 in 40,000 live births, making it a rare entity [2]. It is diagnosed by the simultaneous presence of at least three out of the six VACTERL acronym anomalies without clinical or laboratory evidence suggesting other differential diagnosis [3]. Though first described 40 years ago by Quan and Smith [4] a single unifying cause remains unfound; with the most accepted explanation relating the disorder to developmental field defects during blastogenesis which phenotypically affect multiple organ systems [5,6]. Diagnosis of VACTERL association is primarily clinical, based on the presence of the hallmark anomalies. Its management involves a multidisciplinary approach tailored to the specific anomalies present in each individual, aimed at addressing both immediate and long-term health challenges.
A 30-year - old patient with G3P1L1A at 36 weeks of gestation with kyphoscoliosis, and VSD was identified for emergency LSCS due to preterm labour. She underwent anoplasty at 6 months of age. She had a history of recurrent lower respiratory tract infections. Physical examination revealed short stature (height-120 cm, weight -50 kg), severe thoracolumbar kyphoscoliosis. Airway exam revealed a Mallampati class II airway, 7 cm thyromental distance and intact cervical range of motion. Systemic examination revealed bilateral crackles and a grade III/VI holosystolic murmur along the left sternal border. The electrocardiogram revealed a normal sinus rhythm. A 2D echocardiography revealed an ejection fraction of 65%, a 6 mm apicomuscular VSD with an L->R shunt. X ray thoracolumbar spine showed thoracolumbar curvature is larger and exhibits more rotation with severe thoracolumbar levoscoliosis (Figure 1). Based on the vertebral, anal, and cardiac anomalies, a diagnosis of VACTREL association in parturient was established. After pre-anaesthetic workup and informed consent, she was scheduled for emergency LSCS due to foetal distress. An 18G IV cannula was secured. In the sitting position, spinal anaesthesia was administered via 1.2 cc of hyperbaric bupivacaine and 25 mcg of fentanyl at the L2-L3 space via a paramedian approach with a 25G Quincke’s spinal needle, which was challenging due to anatomical anomalies. Adequate anaesthesia was achieved up to the T6 dermatome. A healthy baby weighing 2.6 kg was delivered with Apgar scores of 8, 9, and 10 at 1, 5, and 10 minutes respectively. For postoperative analgesia, a bilateral transversus abdominis plane block (TAP) was performed under ultrasound guidance.
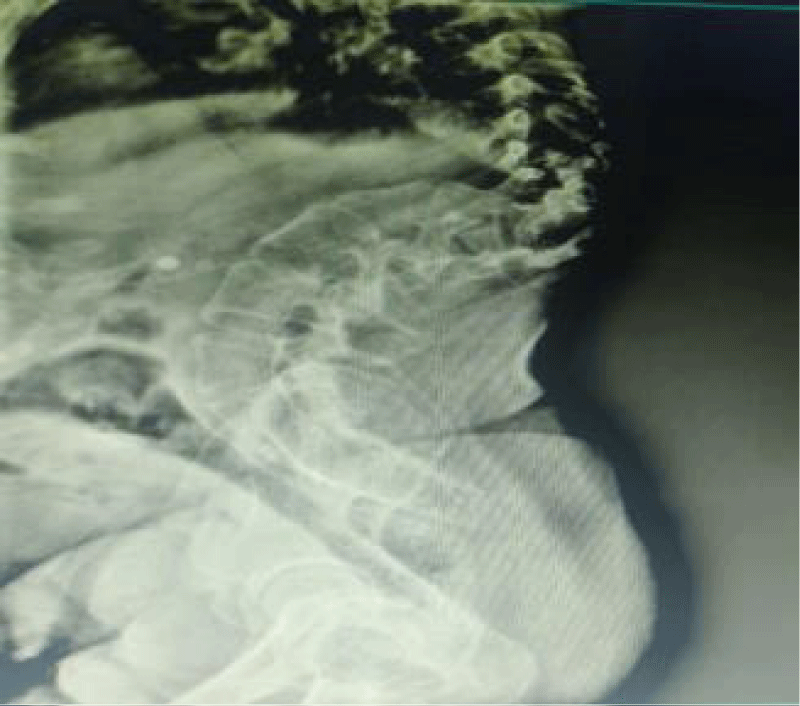
Figure 1: Lateral standing Lateral X-ray of the spine showing severe thoracolumbar kyphoscoliosis.
In 1973, Quan and Smith were the first to describe the VATER association [7]. Temtamy, et al. suggested the inclusion of vascular defects like ventricular septal defect (VSD) and single umbilical artery in the V of VATER association [7]. In 1974, addition of cardiac (C) and limb defects (L) changed the acronym to VACTERL association. Recently VACTERL-H has been described for associated hydrocephalus (H) in the newborn [8]. Its frequency is estimated to be between 1/10,000 and 1/40,000 infants, with approximately 70% male preponderance [9], making it a rarity, especially within the obstetric population.
The etiology of VACTERL association is unknown and many cases occur sporadically. Several authors have suggested that developmental field defects during blastogenesis (2-4 weeks of gestation) may impair the formation of multiple organs simultaneously [10]. Multiple environmental factors like maternal diabetes mellitus, alcohol and teratogenic drugs (sex hormones, anticholestrol drugs, lead, Adriamycin, venlafaxine, anti-epileptic drugs) interact with genetically susceptible genome [10]. Although the exact genetic cause has not been established but several genetic mutations, chromosomal aberrations and mitochondrial defects have been reported in relation to some components of VACTERL association [8].
Vertebral, anal, cardiac, tracheoesophageal, renal and limb anomalies constitute the major components of VACTERL association. In addition to these prime features, patients may also have other congenital anomalies like hydrocephalus, ribs and brachial arch anomalies. Our parturient had the three (cardiac, tracheoesophageal and anal) major components of VACTERL association. Vertebral anomalies are the most frequently reported defects in 60% - 80% cases and they were appreciated in our case [11]. The range vertebral anomalies are broad, and include defects such as hemivertebrae, vertebral fusions, and supernumerary or absent vertebrae and dysplastic vertebrae such as ‘‘butterfly vertebrae’’, ‘‘wedge vertebrae’’. In addition, neurologic anomalies such as Tethered Spinal Cord (TSC), syrinx, tight filum terminale, and lipomeningomyelocele have also been described in patients with colorectal and urogenital abnormalities in VACTERL association, usually with neuro-logic manifestations [12,13]. Renal anomalies are reported in 50% to 80% of the cases in the form of unilateral renal agenesis (absent left kidney in our case), horseshoe, and cystic and/or dysplastic kidneys [14,15]. Cardiac anomalies occur in 50% - 80% of cases further VSD, ASD, (finding of our case) and tetralogy of Fallot are amongst the frequently reported defects [3]. Tracheoesophageal anomalies occur in approximately 50% - 70% of patients and they may be associated with lung anomalies. Limb anomalies are reported in approximately 40% - 55% patients and include radial ray deformities, (absent radius, polydactyly, syndactyly, radioulnar synostosis) club foot, hypoplasia of great toe/tibia and lower limb tibial deformities [14,15].
As VACTERL association is diagnosis of exclusion, so we excluded rare syndromes like Alagille syndrome (no typical facial appearance or ophthalmic anomalies), Baller-Gerold syndrome (no skin anomalies or craniosynostosis), CHARGE syndrome (no coloboma, ear anomalies/facial features), Fanconi’s anemia (no abnormality in pigmentation or hematologic parameters), Feingold’s syndrome (no syndactyly at toes) and Fryns’ syndrome (no diaphragmatic abnormality or facial anomalies) on clinical evaluation and investigative workup [10].
VACTERL is defined as the presence of at least three of congenital malformations, our patient had severe thoracolumbar kyphoscoliosis, VSD and past history of anoplasty. VSD is a common form of congenital heart disease in pregnant women. The aim was to avoid any increase in pulmonary pressures and shunt reversal. Patients with long standing kyphoscoliosis have restrictive lung disease and decrease in FRC and tidal volume. Our options were to choose between general or regional anaesthesia or a combination of both. We were concerned about using a neuraxial block as the primary anaesthetic technique for cesarean delivery for a number of reasons. Literature suggests 25% of patients may experience sensory block extension to cervical dermatomes due to vertebral column anomalies, higher incidence of difficult neuraxial blockade and failure of same. In this case, we avoided general anesthesia due to active LRTI, risk of high airway pressure during ventilation and high intrathoracic pressure can reduce venous return and cardiac output. There was a higher risk of complications from neuraxial anaesthesia in our case for several reasons: There was a risk of inadvertent CSF drainage after a spinal anaesthetic or accidental dural puncture during epidural placement, which could lead to CSF pressure changes and rapidly progressive myelopathy. Hara, et al. reported two such cases wherein a low CSF pressure related to a post-surgical drainage of CSF lead to progressive myelopathy with hyperreflexia of upper limb and hyperalgesia [16].
In the setting of severe restrictive lung disease, neuraxial analgesia may be a viable option for labour and vaginal delivery, however, neuraxial anesthesia during caesarean section may exacerbate respiratory compromise. Another anaesthetic concern with these patients, which was a factor in this case, is the potential for a difficult airway in the setting of skeletal anomalies, including thoracolumbar scoliosis.
A major problem of regional anesthesia is fall in systemic vascular resistance, reversal of shunt and hypoxemia. In our case, we gave minimal dose of hyperbaric bupivacaine and fentanyl to avoid rapid fall in BP. Intraoperative hypotension was managed with bolus dose of phenylephrine.
This case report highlights the importance of multidisciplinary planning, an individualised approach and shared decision making in managing pregnant patients at high risk for perioperative morbidity due to severe congenital anatomical abnormalities. A meticulous preoperative assessment and rigorous intraoperative monitoring contributed to the safe delivery of a patient with VACTERL syndrome.
Ethical considerations
Informed consent was obtained from the patient for both the procedure and the publication of this case report. The authors affirm that the patient’s confidentiality has been maintained. Additionally, a Bonafide Document issued by S. Nijalingappa Medical College & HSK Hospital, Navanagar, Bagalkot -587103 (Reference No: BVVS/SNMC/ANS/2025/480) confirms that this case report is part of routine clinical care and was therefore exempt from additional ethical review under the institution’s policies. The authors take full responsibility for the authenticity of this information.
- Velazquez D, Pereira E, Havranek T. Neonate with VACTERL association and a branchial arch anomaly without hydrocephalus. AJP Rep. 2016;6(1):74-6. Available from: https://doi.org/10.1055/s-0035-1566297
- Bhagat M. VACTERL association-type anomalies in a male neonate with a Y-chromosome abnormality. OMCR. 2015;2015:164-166. Available from: https://doi.org/10.1093/omcr/omu062
- Ramosa JA, Shashank S, Shettarb SS, James CF. Neuraxial analgesia in a parturient with the VACTERL association undergoing labour and vaginal delivery. Rev Bras Anaesthesiol. 2016;343-9.
- Quan L, Smith DW. The VATER association. Vertebral defects, anal atresia, T-E fistula with oesophageal atresia, radial and renal dysplasia: a spectrum of associated defects. J Pediatr. 1973;82:104–107. Available from: https://doi.org/10.1016/s0022-3476(73)80024-1
- Solomon BD. VACTERL/VATER association. Orphanet J Rare Dis. 2011;6:56. Available from: https://doi.org/10.1186/1750-1172-6-56
- Hersh JH, Angle B, Fox TL, Barth RF, Bendon RW, Gowans G. Developmental field defects coming together of associations and sequences during blastogenesis. Am J Med Genet. 2002;110:320-3. Available from: https://doi.org/10.1002/ajmg.10429
- Shaw-Smith C. Genetic factors in oesophageal atresia, tracheo-oesophageal fistula and the VACTERL association: Roles for FOXF1 and the 16q24.1 FOX transcription factor gene cluster, and review of the literature. Eur J Med Genet. 2010;53(1):6-13. Available from: https://doi.org/10.1016/j.ejmg.2009.10.001
- Chen Y, Liu Z, Chen J, Zuo Y, Liu S, Chen W, et al. The genetic landscape and clinical implications of vertebral anomalies in VACTERL association. J Med Genet. 2016;53:431-7. Available from: https://doi.org/10.1136/jmedgenet-2015-103554
- Czeizel A, Ludanyi I. An aetiological study of the VACTERL-association. Eur J Pediatr. 1985;144:331-7. Available from: https://doi.org/10.1007/bf00441773
- Cevik MO, Celik M, Bucak IH, Almis BH, Turgut M. Possible relation of antenatal venlafaxine use and VACTERL association in a newborn: A case report. Turkish J Psychiatr. 2017;28(1):67-70. Available from: https://pubmed.ncbi.nlm.nih.gov/28291300/
- Bjørsum-Meyer T, Herlin M, Qvist N, Petersen MB. Vertebral defect, anal atresia, cardiac defect, tracheoesophageal fistula/oesophageal atresia, renal defect, and limb defect association with Mayer-Rokitansky-Küster-Hauser syndrome in co-occurrence: two case reports and a review of the literature. J Med Case Rep. 2016;10(1):374. Available from: https://doi.org/10.1186/s13256-016-1127-9
- Lawhon SM, MacEwen GD, Bunnell WP. Orthopaedic aspects of the VATER association. J Bone Joint Surg Am. 1986;68:424-9. Available from: https://pubmed.ncbi.nlm.nih.gov/3949837/
- Raam MS, Pineda-Alvarez DE, Hadley DW, Solomon BD. Long-term outcomes of adults with features of VACTERL association. Eur J Med Genet. 2011;54:34-41. Available from: https://doi.org/10.1016/j.ejmg.2010.09.007
- Reddy AKV, Soren C. VACTERL association in a newborn - A rare case report. IOSR J Dental Med Sci. 2017;16(1):31-3. Available from: https://www.iosrjournals.org/iosr-jdms/papers/Vol16-issue1/Version-5/F1601053133.pdf
- Botto LD, Khoury MJ, Mastroiacovo P, Castilla EE, Moore CA, Skjaerven R, et al. The spectrum of congenital anomalies of the VATER association: an international study. Am J Med Genet. 1997;71:8-15. Available from: https://pubmed.ncbi.nlm.nih.gov/9215761/
- Hara T, Nakajima M, Sugano H, Karagiozov K, Miyajima M, Arai H. Cerebrospinal fluid over-drainage associated with upper cervical myelopathy: successful treatment using a gravitational add-on valve in two cases. Interdiscip Neurosurg. 2020;19:100586. Available from: https://doi.org/10.1016/j.inat.2019.100586